
Beyond
willpower.
Sustainable weight loss with GLP-1 protocols, real metabolic data, and expert tuning. Semaglutide, tirzepatide, dose ramps, and the bedrock work that keeps the change after you taper off. When your protocol calls for a prescription, TTL’s telehealth handoff connects you with an independently licensed provider who already has your full picture. Coming soon.
5-minute intake · No credit card · Your plan is yours to keep
Worth a closer look if
- BMI 27+ with weight-related conditions
- BMI 30+ across the board
- Insulin resistance or pre-diabetes
- Stalled, even with diet and exercise dialled in
- Holding the line after rapid weight loss
If a few of these land, the conversation is worth having.
The playbook, before the prescription.
- Bedrock first. Sleep, stress, training, and protein floor handled before any pharmacology layers on top — otherwise you lose muscle along with the fat, and the result is harder to hold.
- Three generations of incretin therapy, explained plainly. Semaglutide (single GLP-1, deepest cardiovascular outcome data), tirzepatide (dual GLP-1/GIP, current best-in-class for weight loss), and retatrutide (triple GLP-1/GIP/Glucagon, Phase 3, anticipated 2026–2027). Mechanism, expected weight-loss range, side-effect profile, and where each fits in your timeline.
- Retatrutide on the horizon. The next-generation triple agonist showed about 22–24% mean weight loss at 48 weeks in Phase 2 (NEJM 2023). Phase 3 readouts and regulatory submission are anticipated 2026–2027. We follow the program so you know the moment it becomes a real, vetted option — and we’re honest about why compounded versions circulating today are not the way to access it.
- Dose-escalation references. Standard ramps, slower-tolerance ramps, and the signals that tell you to slow down.
- A side-effect playbook that meets reality. Nausea, constipation, fatigue, gallbladder considerations, and muscle-preservation strategies — named, not glossed over.
- Metabolic biomarker tracking. A1C, fasting insulin, fasting glucose, lipids, ApoB, lipase — trended in your Codex so you can see what’s actually moving.
- A maintenance roadmap. What to do after you hit your goal so you don’t bounce back — tapering strategies, lifestyle anchors, and the bedrock layer that keeps the change.
- A clinician-ready brief. The questions worth asking, the contraindications worth flagging, and the numbers to bring — so the visit is productive from minute one.
GLP-1 lane · What you walk out with
Your metabolic blueprint, end to end
A blueprint that explains the medicine, tracks the biomarkers that matter, and gets you ready for a clinician visit that actually moves things forward.
Get started →Free 7-day trial · $9.99/mo after · Lane Rx TBA
Three generations · at a glance
-
Semaglutide · single GLP-1
Deepest cardiovascular outcome data; mature evidence base.
-
Tirzepatide · dual GLP-1 / GIP
Current best-in-class for weight loss in head-to-head data.
-
Retatrutide · triple GLP-1 / GIP / Glucagon
~22–24% mean weight loss at 48 weeks in Phase 2 (NEJM 2023). Phase 3 readouts anticipated 2026–2027.
Metabolic biomarkers tracked
All trended in your Codex week over week so you see what’s actually moving — not just the number on the scale.
What this isn’t
We don’t prescribe, ship vials, or push compounded versions of medicines that aren’t cleared yet. The TTL lane gives you the education, the tracking, and the clinician-ready brief — the prescribing belongs with a clinician, on a real medicine, when the timing is right.
For those who refuse to settle for hype.
Tomorrow Today Longevity (TTL) is for those who refuse to settle for hype. You know you need more. You’re tired of chasing trendy peptides, expensive biohacks, and overhyped products that promise the world but deliver disappointing or short-lived results.
We designed TTL for people who want genuine, sustainable longevity outcomes — built on a deep respect for how the human body actually works and structured, evidence-based protocols.
The questions that actually matter.
Before you talk to a clinician, you deserve plain answers — not marketing copy. Here’s what the evidence says.
How much weight can I realistically lose?
~15%
Semaglutide 2.4 mg
68 weeks · STEP 1
~22%
Tirzepatide 15 mg
72 weeks · SURMOUNT-1
~24%
Retatrutide (Phase 2)
48 weeks · NEJM 2023
These are population averages — individual results depend on starting weight, dose tolerated, adherence, and the lifestyle work underneath. Most meaningful change appears in the first 6–9 months. The higher the dose you can tolerate without intolerable side effects, the greater the loss. Tirzepatide is currently best-in-class; retatrutide will likely surpass it once approved.
Will I regain the weight if I stop?
Yes, without a plan. The STEP 1 extension trial showed that participants who stopped semaglutide without structured support regained approximately two-thirds of their lost weight within a year. GLP-1 agonists don’t “cure” obesity — they manage it, like blood pressure medication manages hypertension.
That’s why TTL starts with bedrock (protein floor, resistance training, sleep, metabolic flexibility) before pharmacology. When the foundation is solid, tapering is possible for some people. For others, low-dose maintenance is the right long-term answer. Your plan models both paths.
Typical treatment duration: Most clinicians plan for 12–24 months at therapeutic dose, then reassess. Some patients taper to the lowest effective dose; some stop entirely with careful monitoring; some stay on long-term. There is no universal stop date.
What are the real side effects — and how do you manage them?
| Side effect | Frequency | Management |
|---|---|---|
| Nausea | 40–50% | Slow dose ramp, smaller meals, avoid fatty foods; usually fades by week 4–8 |
| Constipation | 20–25% | Hydration, fiber, magnesium citrate, psyllium |
| Diarrhea | 15–20% | Typically transient during dose escalation |
| Fatigue / low energy | 10–15% | Often from caloric undershoot; protein & meal timing adjustment |
| Gallbladder issues | ~2–5% | Risk increases with rapid weight loss; ursodiol if history; monitor symptoms |
| Pancreatitis (rare) | <1% | Absolute contraindication to continue; lipase monitoring |
Most GI side effects are dose-dependent and improve with time. The key lever is titration speed — a slower ramp means fewer side effects, even if weight loss starts later. Your plan includes the specific signals that tell you (and your clinician) to slow down.
What about muscle loss, “Ozempic face,” and body composition?
“Ozempic face” refers to facial volume loss from rapid subcutaneous fat reduction. It’s not a direct drug side effect — it’s what fast weight loss looks like in the face, particularly in people over 40 with less collagen reserve.
Muscle loss is the real concern. In trials, roughly 25–40% of total weight lost on GLP-1 agonists alone is lean mass. Without intervention, that means weaker bones, lower metabolic rate, and a body that rebounds faster.
How to prevent it:
- Resistance training 3–4x/week (non-negotiable)
- Protein floor: 1.2–1.6 g/kg body weight daily, even when appetite is suppressed
- Creatine monohydrate (5 g/day) for additional lean-mass support
- Slower dose escalation if weight loss exceeds ~1% body weight/week
- DEXA or bioimpedance tracking every 8–12 weeks
This is why TTL’s GLP-1 lane starts with bedrock — the resistance work and protein habit are in place before the pharmacology layers on, so the loss is fat-dominant from day one.
Who should NOT take GLP-1 agonists?
These are absolute or strong relative contraindications your clinician will screen for:
- Personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia type 2 (MEN2)
- History of pancreatitis
- Pregnancy or actively trying to conceive (discontinue at least 2 months before conception for semaglutide; 1 month for tirzepatide)
- Severe gastroparesis or bowel obstruction
- History of eating disorders — appetite suppression can mask or worsen disordered patterns
- Type 1 diabetes (not indicated; risk of DKA complications)
Your TTL intake flags these automatically and includes them in your clinician-ready brief so nothing gets missed during the visit.
Are there benefits beyond weight loss?
Increasingly, yes — and this is where the longevity angle enters:
- Cardiovascular risk reduction. The SELECT trial (2023) showed semaglutide 2.4 mg reduced major adverse cardiovascular events (MACE) by 20% in overweight/obese adults without diabetes. First obesity drug to demonstrate hard CV endpoints.
- Liver health (MASH/NAFLD). GLP-1 agonists significantly reduce liver fat, inflammation markers, and fibrosis scores. Multiple Phase 3 trials are pursuing semaglutide as a MASH therapeutic.
- Systemic inflammation. Reductions in hs-CRP, IL-6, and TNF-alpha observed across trials — driven partly by fat loss and partly by direct receptor effects.
- Neuroprotection (emerging). GLP-1 receptors exist in the brain. Early trials exploring semaglutide for Alzheimer’s and Parkinson’s are underway (EVOKE, Phase 3). Not proven yet, but the signal is real.
- Kidney protection. The FLOW trial (2024) showed semaglutide reduced kidney disease progression by 24% in patients with Type 2 diabetes and CKD.
Your Codex tracks the metabolic markers (ApoB, hs-CRP, A1C, fasting insulin) that capture these benefits beyond the number on the scale.
What does it actually cost — and what about compounded versions?
| Option | Typical cost (US) | Notes |
|---|---|---|
| Wegovy / Ozempic (brand semaglutide) | $900–$1,350/mo | Insurance coverage expanding; manufacturer savings cards available |
| Zepbound / Mounjaro (brand tirzepatide) | $1,000–$1,100/mo | Lilly savings card ($25/mo with commercial insurance) |
| Compounded semaglutide | $150–$500/mo | 503A/503B pharmacy; legal while FDA shortage declared |
| Compounded tirzepatide | $200–$600/mo | Same regulatory status as above; check current shortage status |
On compounded GLP-1s: Compounding pharmacies can legally produce copies of FDA-approved drugs while those drugs are on the official shortage list. This is how most cash-pay telehealth clinics offer semaglutide at $150–$500/month. The tradeoff:
- No Phase 3 bioequivalence testing on the specific compounded batch
- Sterility depends on the individual pharmacy’s practices
- Once the shortage resolves, FDA can (and has announced intent to) stop compounding
- Dosing accuracy varies — some patients report inconsistent responses batch to batch
TTL doesn’t prescribe or sell compounded product. We educate you on the landscape so you make an informed choice with your clinician — eyes open to the risks and the savings.
How does dosing work?
Both semaglutide and tirzepatide use a slow titration (dose escalation) to minimize GI side effects:
Semaglutide
0.25 mg → 0.5 → 1.0 → 1.7 → 2.4 mg/week
Each step: 4 weeks minimum
Full therapeutic dose by ~month 5
Tirzepatide
2.5 mg → 5 → 7.5 → 10 → 12.5 → 15 mg/week
Each step: 4 weeks minimum
Full therapeutic dose by ~month 5–6
Your TTL plan includes a tolerance-guided ramp: stay at each dose until side effects are manageable before stepping up. If nausea is severe, the plan flags a slower schedule (6–8 week steps) and the signals worth discussing with your clinician before the next escalation.
Three tiers. No surprises.
Start free, subscribe for your lane at $9.99/mo, or unlock all five lanes with TTL at $14.99/mo. Add prescription support when our clinician network is live.
Free trial
$0
/ 7 days
A peek inside
Take the intake, pick your lane, generate your first plan. After 7 days the trial ends unless you subscribe.
Start free trial →No credit card to start
App subscription
$9.99
/ month
or $79/yr · save 34%
1 lane, full app
Pick one lane and get everything you need — 25-expert AI panel, refinements, weekly Codex updates, tracker, lab uploads, wearable sync. Upgrade to TTL ($14.99/mo) for all 5 lanes + advanced features.
SubscribeCancel anytime · US & MX
Lane Tele/Rx
TBA
preview
TTL + telehealth + Rx
Everything in App, plus telehealth match with a licensed metabolic clinician in your state and prescription support for tirzepatide (current best-in-class) or semaglutide, with safe dose-escalation oversight. Retatrutide added once Phase 3 readouts and supply mature.
Notify meFinal pricing announced before launch
All prices in USD. App subscription ($9.99/mo) covers 1 lane. TTL subscription ($14.99/mo) unlocks all 5 lanes + advanced features. Lane Tele/Rx adds telehealth + prescription handoff when our clinician network goes live.
A look at your Codex Analysis
Initial · Week · Goal — your starting baseline, this week's substrate score, and where the plan takes you. Refreshed weekly as you bring more data.
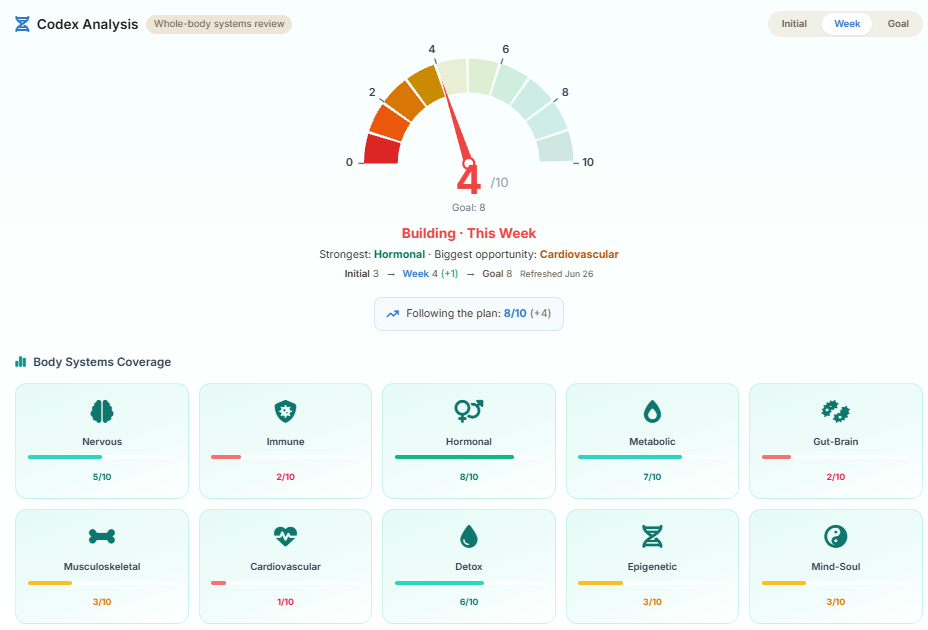
Illustrative preview. Your numbers reflect the labs, deep-dives, routines, and lifestyle data you've shared.
See it on the Sample AccountThe more you bring, the truer the picture.
Your Codex score is dynamic. It starts sparse on day one and climbs every week as you bring more substrate — labs, deep-dive answers, confirmed routines, and wearable data. The Goal is the destination; the work is the partnership.
Initial → Week → Goal
Your Initial score reflects what we know on day one — usually sparse. Each lab you upload, deep-dive you complete, and routine you confirm lifts your Week score toward your Goal. Refreshed every week.
- Upload labs — we parse them and trend each biomarker.
- Complete deep-dives — targeted Q&A with each expert.
- Confirm weekly routines — one tap, the loop closes.
- Connect a wearable — passive substrate, no extra effort.
After intake: More Info Needed
The intake is short on purpose. After it, we open your blueprint and show More Info Needed tiles — Required first, then Revisit, Optional, Beneficial, and Protocol Review Due. Your full plan generates once the required tiles are done.
- Required — we genuinely need it to plan accurately.
- Revisit / Optional — sharpens the plan, not blocking.
- Beneficial — further personalization when you have time.
Pyramid is the path. Codex is the result.
The TT Longevity Pyramid is the visual of the work needed to reach full optimization — Bedrock first, then Testing, Therapies, and Next Level. Your Codex Analysis is the result of progressing along that path: the score that climbs as each tier of the pyramid fills in.
Think of the pyramid as the recipe and the Codex as the dish — the score reflects how much of the recipe you’ve actually completed.
A 25-expert AI panel behind every plan.
Your lane plan is built by the same 25-expert panel that runs the full TTL Codex. Each specialist contributes within their field, the orchestrator reconciles overlap, and the result is a single coherent protocol that updates as you bring more data.
Chief Longevity Architect
Plan design + protocol orchestration
Longevity Science
Epigenetics, NAD+, age-reversal biology
Regenerative Medicine
Stem cells, exosomes, peptide therapy
Metabolic & Fasting
Glucose, lipids, weight, GLP-1, fasting
Precision Nutrition
Personalised diet, blood-type, hydration
Cellular Reset & Senolytics
Senescent cell clearance, fasting
Hormone, Mitochondrial & Energy
TRT, HRT, mitochondrial support
Neuro-Somatic Resilience
Stress, sleep, trauma, nervous system
Emerging Technologies
Reprogramming, gene therapy, AI labs
Oncology & Advanced Therapeutics
Cancer screening, IV therapeutics
Master Peptide Architect
BPC-157, GHK-Cu, GLP-1 micro-dosing
Precision Diagnostics
Lab interpretation, biomarker tracking
Integrative & Plant Medicine
Adaptogens, herbs, holistic protocols
Aesthetic Regeneration
Skin, hair, body composition
Panel Orchestrator
Convergence + plan reconciliation
10 sub-specialists who join your panel when your case requires them — men’s health, women’s HRT, trauma & mind-body, immuno-oncology, Codex systems integration, and more.
They converge.
After your intake, every expert reviews your substrate within their specialty. The orchestrator reconciles overlap, resolves conflicts, and produces one coherent plan — not 25 parallel chatbot answers.
They reconvene.
Every lab you upload, deep-dive you complete, routine you confirm, or wearable sync brings the panel back together. The plan refines, your Week Codex score climbs toward your Goal.
Ask any one of them.
Subscribers can chat 1:1 with any expert to discuss something that matters to you. Then if desired, the outcome of the conversation can be added to your plan with one click. This is real personalization!
How we keep this honest.
Six commitments we hold ourselves to. They're also why we look different from the clinics.
Independent
No formulary, no kickbacks, no compounds for sale. Your protocol is the one that fits, not the one we're paid to push.
Encrypted at rest
PHI columns are encrypted at the application layer (AES-128 + HMAC) with a key held in our hosting provider’s encrypted secret store, separate from the database. Logs never contain raw PHI.
No data sales, no ads
We don't sell, rent, or trade your data. We don't run ads. Our revenue is the subscription you pay us — that's the entire business.
Independent guidance
High-quality health and wellness information intended to support informed decision-making. We give you the protocol; the prescription stays with your doctor.
Export & delete anytime
Your data is yours. Export it as JSON or delete your account in one click — we honor a 30-day undelete in case you change your mind.
US & MX coverage
Telehealth matched to where you live, units in your system (lb/kg, ft·in/cm, oz/ml).
Built for people who've outgrown spreadsheets.
You already know your TSH, your hs-CRP, and your VO₂ max. You've tried the apps, the wearables, and a notebook or two. TTL is the next step — a structured, expert-built protocol that connects what you're already tracking to what your plan should actually look like.
-
You ask better questions than your doctor's intake form does. So we ask better ones.
-
You want the protocol AND the reasoning. Every recommendation cites the mechanism and the evidence tier.
-
You'd rather pay $9.99/mo than be the product. No data sales, no ads, no upsell kickbacks.
Reset your metabolism — properly.
Five minutes of intake. Real medicine education. A clinician-ready blueprint that includes the side-effect playbook, the biomarkers worth tracking, and the bedrock work that holds the change after you taper. Free to start.