Through every
season.
Personalized HRT protocols built on your symptoms, your labs, your goals. Estradiol, progesterone, timing, and the science that decides how the next thirty years feel. When your protocol calls for a prescription, TTL’s telehealth handoff connects you with an independently licensed provider who already has your full picture. Coming soon.
5-minute intake · No credit card · Your plan is yours to keep
Sound familiar?
Signs HRT might be worth a conversation.
- Hot flashes or night sweats
- Sleep that no longer holds, anxiety, mood shifts
- Brain fog, words that don’t come
- Low libido, vaginal dryness
- Joints that ache, weight that won’t move
A few of these is enough to start looking. You don’t need every symptom on the list.
Build my HRT blueprint →Independent guidance · Free trial intake
The 3 questions that actually decide it
“Is it safe for me?”
For most women under 60 or within 10 years of menopause, benefits outweigh risks. Family history doesn’t automatically rule it out — it changes the conversation, not the answer.
“Will I actually feel better?”
Hot flashes drop 75–90% within 4–8 weeks. Sleep improves in 2–4 weeks. Mood, fog, and libido follow. Most women feel meaningfully different within the first month.
“What if I want to stop?”
No universal stop date. Taper gradually over 3–6 months. ~50% get milder symptoms back. You’re not “dependent” — HRT replaces what your body used to make.
The 10-year window.
When you start HRT matters more than whether you start. Women who begin within 10 years of menopause — or before age 60 — see the most favourable balance of benefits across bone, brain, heart, and overall mortality. After that window, the math changes. Starting HRT past 65 has been linked to higher Alzheimer’s risk in meta-analyses, while women who start within 5 years of menopause see up to 32% lower risk.
The 2002 Women’s Health Initiative reported HRT risks in women who were on average 63 years old and well past menopause — far past the window we now know matters most. It took the field two decades to fully revisit those findings. The long-term WHI follow-ups, the NAMS 2022 position statement, and the FDA’s November 2025 removal of the estrogen black-box warning have put the conversation back where it belongs: timing, formulation, and your individual risk profile.
In practice, perimenopause is when this conversation usually begins. The 10-year clock officially starts at your final period — but the protective window opens earlier, when symptoms first show up and the ovary is winding down. Knowing where you are on that arc is half the decision. The other half is a conversation with a clinician who knows you, looking at the numbers and the life you actually want.
How TTL helps
TTL maps your stage, reads your labs in plain English, and gathers the right questions to ask — so when you sit down with a clinician, you don’t start from scratch. Lane Rx (coming soon) will match you with a licensed physician in your state when prescribing is the right next step.
Hormone-protection window
-
Late 30s Late 30s
Build Build runway
-
Peri Perimenopause
Opens Window opens
-
Meno Menopause
Optimal Optimal start
-
+10y 10y post-meno
Open Window still open
-
60+ Past 60
Diff. Different protocol
Source: NAMS 2022 position statement; WHI 10-year follow-up. Educational summary, not medical advice.
What relief looks like
Most women notice meaningful improvement within 4–8 weeks.
Response is individual. If symptoms are mild, your blueprint also surfaces non-hormonal strategies (lifestyle, adaptogens, phytoestrogens) that may be enough on their own.
Common perimenopause signals
Three or four is enough to start the conversation — trust what your body is telling you.
- Cycle length changing
- Hot flashes / night sweats
- Sleep disruption
- Mood + anxiety shifts
- Brain fog / memory lapses
- Joint aches, dryness
- Lower libido
- Belly-fat redistribution
Five systems. One intervention.
Estradiol does much more than regulate periods. When it falls at menopause, five systems lose a chemical signal they’ve relied on for decades — bone, heart, brain, muscle, and metabolic health all start to shift at once. The good news: HRT, started in the right window, can soften that shift across every one of them.
Bone
-30 to -50% fracture risk
HRT preserves bone density. The single most well-studied HRT benefit.
Heart
#1 cause of death in women
Started in the window, HRT is linked to better cardiovascular outcomes.
Brain
Up to -32% Alzheimer’s risk
Meta-review: HRT within 5 years of menopause. After 65, the risk profile reverses.
Muscle
Estrogen ↔ muscle protein synthesis
Estradiol falls speed up sarcopenia. HRT plus strength training is what shifts it.
Metabolic
Insulin sensitivity, fat distribution
HRT modestly improves how the body handles glucose and shifts where fat is stored.
Bone
The most well-studied HRT benefit.
Estradiol holds back the cells that break down bone. When it falls at menopause, women lose 2-3% of bone mass per year for several years — cumulative loss reaches 30-40% over a lifetime, and one in two women over 50 will fracture a bone at some point. Multiple randomized trials and the NAMS 2022 statement support HRT as effective primary prevention for postmenopausal osteoporosis, with fracture risk down 30-50% when started in the window. Bone density gains plateau over time, but that risk reduction holds for as long as therapy continues.
Sources: NAMS 2022 Position Statement; WHI 18-year follow-up (JAMA 2017); USPSTF 2022.
Heart
The leading cause of death in women — and timing changes the picture.
Heart disease takes more women’s lives than every cancer combined, and the risk climbs sharply after menopause as estradiol’s protective effect on blood vessels fades. The 2002 WHI study that scared the field looked at women in their 60s, with arteries that had already aged. Newer analyses by age group tell a different story: women who start within 10 years of menopause see better cardiovascular outcomes. Women who start after 60 don’t. Delivery method matters too — a patch or gel goes through skin instead of the liver, which carries a lower clot risk than a pill.
Sources: WHI Re-analyses (NEJM 2003, 2007); ELITE trial (NEJM 2016); NAMS 2022.
Brain
Two-thirds of Alzheimer’s patients are women.
The female brain depends heavily on estradiol — it shapes how neurons connect, how the brain uses glucose, and how amyloid (the Alzheimer’s-related protein) gets cleared. A woman’s lifetime Alzheimer’s risk is roughly 1 in 5; for men it’s 1 in 10. Living longer doesn’t fully explain the gap. A review of 50 studies found Alzheimer’s risk up to 32% lower in women who started HRT within 5 years of menopause; the same review found risk 38% higher when HRT began after 65. The CARE initiative is now tracking biomarkers in 100 million women to nail down exactly why.
Sources: Cochrane Review 2017; Mosconi et al. (Neurology 2021); CARE Initiative 2025.
Muscle
Estradiol supports muscle protein synthesis.
Sarcopenia — age-related muscle loss — speeds up sharply at menopause. Women lose 1-2% of lean mass per year through perimenopause, with matching losses in strength and power. Estradiol receptors sit on skeletal muscle, where the hormone helps activate the cells that build new muscle and the mitochondria that fuel it. HRT alone won’t build muscle for you. What it does is take the brake off. Strength training is the gas pedal. Together they preserve what the women’s longevity field has started calling the "organ of longevity" — not for how it looks, but for what it does.
Sources: Maltais et al. (Mol Cell Endocrinol 2009); Lyon "Forever Strong" (2024); GWS Trend #1 2026.
Metabolic
Insulin sensitivity, where fat is stored, how you sleep.
When estradiol falls, fat starts to move from hips and thighs to the belly. That belly fat is metabolically active and inflammatory — it tracks with rising fasting insulin, higher triglycerides, and higher hs-CRP. Combined with menopausal sleep that no longer holds (which itself makes glucose harder to handle), the metabolic picture can worsen even if the scale doesn’t move. HRT modestly improves how the body uses insulin and reverses some of the belly-fat shift. Whether that’s enough to change long-term metabolic risk is still being studied. Strength training, sleep, and protein remain the foundation.
Sources: Salpeter et al. (Diabetes Obes Metab 2006); ELITE substudy 2017; Endocrine Society 2015.
The ovary is command central.
The ovary isn’t only a fertility organ. It runs a signalling network that touches bones, brain, heart, immune system, and metabolism — and it ages about 2.5 times faster than the rest of your body. That’s why the years around ovarian decline change so much, so quickly. It isn’t in your head. The biology has actually shifted.
AMH (Anti-Müllerian Hormone) is the most consistent marker of ovarian reserve we have across a woman’s life. Tested annually from your 30s on, it tells you where you are on the curve and how much time you have to plan.
For decades women were taught the ovary was just a fertility organ — relevant for pregnancy, irrelevant after. The science says the opposite. The ovary is an endocrine organ, conducting a signalling network that reaches bone, brain, heart, immune function, and metabolism. When it stops, every system it was talking to gets quieter at the same time. As Piraye Beim, MD (Celmatix) puts it: "The end of ovarian function is the single biggest accelerant of unhealthy aging in women."
Anti-Müllerian Hormone (AMH), made by small follicles in the ovary, is the most consistent marker of ovarian reserve across a woman’s life. Test once in your late 20s or early 30s to set a baseline — before that, values fluctuate too much to mean much — then annually from your mid-30s on. AMH isn’t a fertility predictor (it doesn’t do that well), but it’s a strong indicator of where you are on the ovarian-aging curve. Falling values usually show up about 5 years before menopause.
The wider field is moving fast. The $50 million XX Prize launched in 2026 to advance ovarian biomonitoring; labs at Columbia, Yale, and the Buck Institute are testing rapamycin, AMH-mimicking drugs, ovarian stem-cell implants, and tissue cryopreservation as ways to slow ovarian aging itself. None of those are clinical-grade yet — but the testing-and-tracking layer (AMH, AFC, follicular monitoring) is here today, and it’s the foundation of a longevity-first protocol.
AMH · illustrative decline curve
> 2.0 ng/mL
Normal reserve. Time to lay the groundwork.
0.5–2.0 ng/mL
Reserve is declining. Worth planning ahead.
< 0.5 ng/mL
Late-perimenopause signal. A timing conversation makes sense.
Where the field is moving
- XX XX Prize ($50M, 2026). A decoder competition aimed at ovarian biomonitoring — hunting the next AMH-quality biomarkers.
- PB Piraye Beim, MD · Celmatix. Reframing the ovary as the conductor of women’s endocrine signalling; AMH-mimicking therapeutics in development.
- JG Jen Garrison, PhD · Buck Institute. Geroscience of the ovary — rapamycin, follicle preservation, and slowing the clock itself.
- JJ Jamie Justice, PhD · XPRIZE Healthspan. Treating ovarian aging as an upstream lever for women’s healthspan, not a downstream symptom.
- CR CARE Initiative. Tracking biomarkers in 100M women to settle the menopause ↔ Alzheimer’s mechanism.
These programs are still in research — not on the TTL plan menu yet. The piece you can act on today is the testing-and-tracking layer: AMH, antral follicle count, your symptom diary.
The synergy triangle
What 1.6 g protein per kg actually looks like
60 kg / 132 lb
96 g
protein / day
70 kg / 154 lb
112 g
protein / day
80 kg / 176 lb
128 g
protein / day
A palm of …
Chicken breast
~30 g
Greek yogurt (1 c)
~20 g
Cottage cheese (1 c)
~25 g
Salmon fillet
~25 g
Spread protein across 3-4 meals. Hitting roughly 3 g of leucine per meal is what tells your muscles to actually use it — and it matters more, not less, after 40.
Strength is no longer optional.
When estradiol falls, muscle and bone start to slip together. Strength training is what slows that slide — it isn’t an add-on at this stage, it’s the foundation. Women who strength-train two or three times a week show roughly 30% lower risk of death from heart disease. That’s a population-level number most medications would envy.
- About 1.6 g of protein per kg of body weight, every day.
- Compound lifts: squat, hinge, push, pull, carry.
- Creatine 3–5 g per day — growing evidence in brain and bone, not just muscle.
- Sleep 7–9 hours. Recovery is where the rebuilding happens.
Dr. Gabrielle Lyon coined the term "musclespan" for the years you live with healthy skeletal muscle. The reframe matters: muscle isn’t about how you look in a sleeveless top. It’s an organ system that regulates blood sugar, helps you stay on your feet, and (in women particularly) protects the bones that hormone loss is quietly thinning. A Cedars-Sinai study found women who strength-trained 2-3 times a week had roughly 30% lower risk of death from heart disease — a number that beats most pharmacotherapy at a population level.
Illustrative · 3 days per week
Day 1 · Lower
Squat · Hinge · Loaded carry
Day 2 · Upper
Push · Pull · Core
Day 3 · Full
Compound mix · Power · Conditioning
A starting framework, not a prescription. Your blueprint adapts to your level, your joints, and your goals — and a trainer or PCP can fine-tune it to your equipment and history.
Sources: Cedars-Sinai cohort (BJSM 2022); Lyon "Forever Strong" (2024); GWS Trend #1 (2026).
Different decade, different priorities.
Women’s longevity follows the ovary, not a single midlife event. The right priorities at 38 aren’t the right priorities at 58. A blueprint that meets you where you actually are — your biology, your symptoms, your decade — will always outperform a generic template.
Late 30s
Lay the groundwork
Most women won’t hit perimenopause for another 5-15 years — and that lead time is the most useful thing you’ll have. Get an AMH baseline (it only becomes meaningful as a multi-year trend, so the earlier you start, the better the picture). Get a DEXA so you know your starting bone density. Start building the strength you’ll lean on later. The metabolic foundation you put down now is what decides how perimenopause actually feels when you get there.
- Establish AMH baseline + DEXA.
- Build muscle. Optimize sleep + stress.
- Annual labs from here on.
Track
AMH, hs-CRP, fasting insulin, DEXA.
Ask your clinician
- ·What does my AMH baseline tell us about my reserve?
- ·Should I get a DEXA scan now to set a baseline?
- ·Are my hs-CRP and fasting insulin in target?
Perimenopause
The window opens
Cycles become unpredictable, sleep thins out, and mood, memory, and metabolism all start shifting — usually before periods stop entirely. This is when the protective HRT window opens. Track your cycle and your symptoms on purpose, get hormonal labs read in context (FSH alone can mislead — it pulses), and start the timing conversation with a clinician you trust. Adding strength volume here pays back twice: once for muscle, once for bone.
- Track cycle, mood, sleep, hot flashes.
- Discuss HRT timing with clinician.
- Increase strength volume.
Track
Estradiol, FSH, LH, AMH, thyroid.
Ask your clinician
- ·Am I in early or late perimenopause based on my labs and symptoms?
- ·When is the right time for me to start HRT, given my history?
- ·Should we trial transdermal estradiol + cycled progesterone?
Menopause
The optimal HRT window
Twelve months without a period is the official line for menopause. The decade that follows is when HRT delivers the most — bone, brain, and cardiovascular protection in addition to symptom relief. The choices that matter here are individual: transdermal or oral, paired with progesterone if you still have a uterus, sometimes a women’s-dose of testosterone for energy and libido. Strength training and adequate protein move from optional to essential at this stage, not negotiable.
- Bone, brain, heart protection priorities.
- Individualized HRT prescription.
- Strength + cardio + protein non-negotiable.
Track
Lipid panel, A1c, DEXA, breast/pelvic.
Ask your clinician
- ·Is transdermal or oral the right delivery for my risk profile?
- ·Do I need cycled or continuous progesterone?
- ·Would low-dose testosterone help my energy and libido?
Post-menopause
Maintain, track, reassess
Past the 10-year mark, the question shifts from "when do I start" to "should I continue, and at what dose?" There’s no universal stop date — the right answer depends on your symptoms, your lab trends, your family history, and the benefit-risk balance that’s specific to you. Cognition and mobility move to the centre of the picture. ApoB, hs-CRP, and a DEXA every one to two years are how you know whether your trajectory is holding.
- Continue HRT if benefit > risk.
- Reassess every 1–2 years with clinician.
- Cognition + mobility focus.
Track
DEXA, ApoB, hs-CRP, cog screening.
Ask your clinician
- ·Should I continue HRT given my current symptom and lab profile?
- ·Is my ApoB on track? Do I need additional cardio-protection?
- ·When should we re-DEXA and re-screen for cognitive trajectory?
Stage is biological, not chronological — your AMH, your FSH, and your symptom pattern place you on this map, not your birthday. TTL reads your stage from intake; the Lane Rx handoff (coming soon) connects you with a licensed clinician for the prescribing decision.
A protocol built for you, watched over time.
HRT isn’t one-size-fits-all. Estrogen is paired with progesterone for safety when there’s a uterus involved. A patch and a pill carry different risk profiles. Women’s-dose testosterone is genuinely dose-sensitive. The standard cadence: a closer look every quarter through your first year, then annually.
Delivery method changes the risk profile. Oral estrogen passes through the liver first, which slightly raises clot risk. Transdermal options — patches, gels, sprays, creams — absorb through skin instead, and skip that first liver pass. If you have a uterus, estrogen is paired with progesterone (cycled or continuous) to protect the endometrium; bioidentical micronized progesterone is the most studied option. A women’s-dose of testosterone (roughly a tenth of a man’s dose) helps energy and libido for some women; current guidelines support testosterone for hypoactive sexual desire disorder once other causes have been ruled out.
The standard contraindications: a personal history of breast cancer, untreated endometrial cancer, active liver disease, a recent stroke or heart attack, or a high baseline clotting risk. Family history matters in the conversation, but it doesn’t automatically rule HRT out. Year one is closer-touch: a baseline panel and symptom diary, a recheck at month 3, a dose adjustment around month 6, and a full re-evaluation at month 12. After year one, annual labs with quarterly symptom check-ins is the typical rhythm.
Normal in the first 1–3 months
Most women experience some adjustment effects that resolve on their own. These are signs your body is responding — not signs something is wrong:
- Breast tenderness
- Light spotting or bleeding
- Mild bloating
- Headaches
- Mood shifts (usually up)
- Nausea (oral only)
If these persist past 3 months, it usually means the dose or delivery method needs adjusting — not that HRT isn’t for you. Your TTL plan includes a side-effects timeline so you know what’s expected vs. what needs a call.
Ask your clinician
- ·Given my history, is transdermal estradiol the safer first choice?
- ·Should we use micronized progesterone, and cycled or continuous?
- ·Is a low-dose testosterone trial appropriate for my libido or energy goals?
- ·What contraindications in my history should we re-screen for first?
- ·How will we monitor — labs, symptom diary, DEXA — and how often?
Educational summary only. TTL doesn’t prescribe — every clinical decision belongs with a qualified clinician. Lane Rx (coming soon) will pair you with a licensed physician in your state when prescribing is the right next step.
Typical baseline panel
Delivery methods at a glance
Oral
- +Convenient daily pill.
- +Lowers LDL modestly.
- −First-pass liver effect.
- −Slightly higher clot risk.
Transdermal
- +Skips first-pass liver.
- +Lower clot + stroke signal.
- +Patch, gel, spray, or cream.
- −Skin reaction in some users.
Progesterone (if you still have a uterus)
Bioidentical micronized, taken at bedtime; cycled or continuous.
Testosterone (women’s dose)
Roughly a tenth of a male dose; off-label for low desire when other causes are ruled out.
Monitoring cadence
Month 0
Baseline + start
Month 3
Symptom + lab recheck
Month 6
Dose tune
Month 12
Annual review
Education today. A real clinician, when you’re ready.
Your TTL blueprint is the prep work — your stage, your labs, your symptom history, the questions worth asking, and a protocol summary a clinician can read in two minutes. Lane Rx (coming soon) will match you with a physician licensed in your state, with your blueprint already in their hands.
Build your blueprint
Free intake. Your stage, your labs, your protocol summary — in your hands.
Track and tune
Logs, labs, and biomarker trends build a real picture across your cycle.
Lane Rx handoff
Coming soon. Matched with a licensed physician in your state, with your blueprint already loaded.
Is HRT right for me?
This isn’t a diagnosis. It’s a thinking framework — a way to organize where you stand before the clinician conversation.
Likely a good fit
- Under 60, or within 10 years of menopause
- Symptomatic: flashes, sleep, mood, fog
- No personal history of breast cancer
- No recent stroke, heart attack, or clot
Worth exploring
- Mild symptoms — lifestyle changes might suffice
- Family history but no personal history
- Interested but nervous — want more info
- Considering non-hormonal options first
Talk to your clinician first
- Personal breast cancer history
- Active liver disease
- Recent cardiovascular event
- High clotting risk (unmanaged)
Even in the third column, HRT isn’t always ruled out — it means the conversation needs to happen with a specialist. Your TTL blueprint captures your full history so you walk in prepared, not guessing.
Sources & citations
- NAMS 2022 Position Statement on Hormone Therapy.
- Women’s Health Initiative (WHI) follow-ups, JAMA 2017 (18-yr) and JAMA 2024.
- USPSTF 2022 Recommendation Statement on Hormone Therapy for Primary Prevention.
- FDA, November 2025 — Removal of black-box warning on most estrogen products.
- Salpeter SR et al. — Diabetes, Obesity & Metabolism, 2006.
- ELITE Trial — NEJM 2016, with metabolic substudy 2017.
- Cochrane Review — HRT and dementia risk, 2017.
- Mosconi L et al. — Neurology 2021, female brain estradiol pathway.
- CARE Initiative (Cutting Women’s Alzheimer’s Risk through Endocrinology), 2025.
- Maltais ML et al. — Mol Cell Endocrinol 2009, estradiol · muscle.
- Lyon G — "Forever Strong" (2024), musclespan framework.
- Cedars-Sinai cohort — BJSM 2022, women + strength training mortality.
- Endocrine Society 2015 — metabolic effects of estrogen therapy.
- Beim P (Celmatix) · Garrison J (Buck Institute) · Justice J (XPRIZE Healthspan) — Global Wellness Institute Wellness Roundtable, 2025.
- XX Prize — $50M ovarian-decoder competition launched 2026.
- Global Wellness Summit — "Future of Wellness 2026 Trends," Trend #1.
TTL summarizes peer-reviewed literature, position statements, and product labelling for educational use. Citations are accurate to the best of our research at the time of publication; please consult the primary sources before any clinical decision.
Four steps. Roughly seven minutes.
Tell us where you are
Cycle history, symptoms, goals — answer what applies, skip what doesn’t.
Add your labs
Estradiol, progesterone, FSH, LH, testosterone, thyroid, vitamin D — from any provider. We’ll read them and track the trend.
Read your blueprint
A 25-expert AI panel builds a personalized protocol around your stage, symptoms, and goals — foundations first, hormones second.
Talk to a clinician
Coming soon. When prescribing is the right next step, we’ll match you with a telehealth provider licensed in your state.
What you’ll actually get.
- Foundations first. Sleep, stress, and recovery come before any hormone protocol — depleted bodies don’t respond to hormones the way rested ones do.
- Estradiol options, explained. Cream, patch, troche, gel — the differences and trade-offs, in language you can use with your clinician.
- Progesterone, in context. Oral or topical, cycled or continuous, and why pairing matters when the uterus is still intact.
- Women’s-dose testosterone. What the research supports, what dose ranges look like, and which labs to watch.
- Lab results that make sense. Your full panel, read and trended, with plain-English explanations of each number.
- Codex hormone view. Every value tracked across your cycle and protocol, alongside how you’re actually feeling and what your wearable shows.
- Questions worth bringing in. The specific things to ask — and the numbers to bring — so the appointment doesn’t start from zero.
HRT lane · What you get
Personalized protocol & tracking
Build your hormone blueprint, understand your labs, track symptoms across your cycle, and walk into your clinician conversation ready.
Get started →Free 7-day trial · $9.99/mo after · Lane Rx TBA
For those who refuse to settle for hype.
Tomorrow Today Longevity (TTL) is for those who refuse to settle for hype. You know you need more. You’re tired of chasing trendy peptides, expensive biohacks, and overhyped products that promise the world but deliver disappointing or short-lived results.
We designed TTL for people who want genuine, sustainable longevity outcomes — built on a deep respect for how the human body actually works and structured, evidence-based protocols.
Three tiers. No surprises.
Start free, subscribe for your lane at $9.99/mo, or unlock all five lanes with TTL at $14.99/mo. Add prescription support when our clinician network is live.
Free trial
$0
/ 7 days
A peek inside
Take the intake, pick your lane, generate your first plan. After 7 days the trial ends unless you subscribe.
Start free trial →No credit card to start
App subscription
$9.99
/ month
or $79/yr · save 34%
1 lane, full app
Pick one lane and get everything you need — 25-expert AI panel, refinements, weekly Codex updates, tracker, lab uploads, wearable sync. Upgrade to TTL ($14.99/mo) for all 5 lanes + advanced features.
SubscribeCancel anytime · US & MX
Lane Tele/Rx
TBA
preview
TTL + telehealth + Rx
Everything in App, plus telehealth match with a licensed HRT-friendly clinician in your state and prescription support for estradiol, progesterone, and testosterone protocols.
Notify meFinal pricing announced before launch
All prices in USD. App subscription ($9.99/mo) covers 1 lane. TTL subscription ($14.99/mo) unlocks all 5 lanes + advanced features. Lane Tele/Rx adds telehealth + prescription handoff when our clinician network goes live.
A look at your Codex Analysis
Initial · Week · Goal — your starting baseline, this week's substrate score, and where the plan takes you. Refreshed weekly as you bring more data.
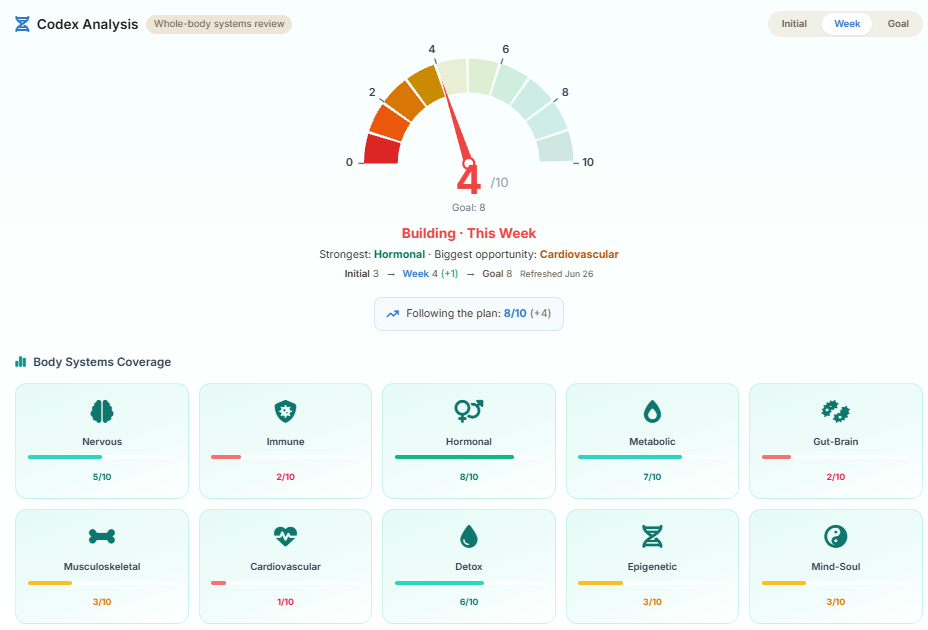
Illustrative preview. Your numbers reflect the labs, deep-dives, routines, and lifestyle data you've shared.
See it on the Sample AccountThe more you bring, the truer the picture.
Your Codex score is dynamic. It starts sparse on day one and climbs every week as you bring more substrate — labs, deep-dive answers, confirmed routines, and wearable data. The Goal is the destination; the work is the partnership.
Initial → Week → Goal
Your Initial score reflects what we know on day one — usually sparse. Each lab you upload, deep-dive you complete, and routine you confirm lifts your Week score toward your Goal. Refreshed every week.
- Upload labs — we parse them and trend each biomarker.
- Complete deep-dives — targeted Q&A with each expert.
- Confirm weekly routines — one tap, the loop closes.
- Connect a wearable — passive substrate, no extra effort.
After intake: More Info Needed
The intake is short on purpose. After it, we open your blueprint and show More Info Needed tiles — Required first, then Revisit, Optional, Beneficial, and Protocol Review Due. Your full plan generates once the required tiles are done.
- Required — we genuinely need it to plan accurately.
- Revisit / Optional — sharpens the plan, not blocking.
- Beneficial — further personalization when you have time.
Pyramid is the path. Codex is the result.
The TT Longevity Pyramid is the visual of the work needed to reach full optimization — Bedrock first, then Testing, Therapies, and Next Level. Your Codex Analysis is the result of progressing along that path: the score that climbs as each tier of the pyramid fills in.
Think of the pyramid as the recipe and the Codex as the dish — the score reflects how much of the recipe you’ve actually completed.
A 25-expert AI panel behind every plan.
Your lane plan is built by the same 25-expert panel that runs the full TTL Codex. Each specialist contributes within their field, the orchestrator reconciles overlap, and the result is a single coherent protocol that updates as you bring more data.
Chief Longevity Architect
Plan design + protocol orchestration
Longevity Science
Epigenetics, NAD+, age-reversal biology
Regenerative Medicine
Stem cells, exosomes, peptide therapy
Metabolic & Fasting
Glucose, lipids, weight, GLP-1, fasting
Precision Nutrition
Personalised diet, blood-type, hydration
Cellular Reset & Senolytics
Senescent cell clearance, fasting
Hormone, Mitochondrial & Energy
TRT, HRT, mitochondrial support
Neuro-Somatic Resilience
Stress, sleep, trauma, nervous system
Emerging Technologies
Reprogramming, gene therapy, AI labs
Oncology & Advanced Therapeutics
Cancer screening, IV therapeutics
Master Peptide Architect
BPC-157, GHK-Cu, GLP-1 micro-dosing
Precision Diagnostics
Lab interpretation, biomarker tracking
Integrative & Plant Medicine
Adaptogens, herbs, holistic protocols
Aesthetic Regeneration
Skin, hair, body composition
Panel Orchestrator
Convergence + plan reconciliation
10 sub-specialists who join your panel when your case requires them — men’s health, women’s HRT, trauma & mind-body, immuno-oncology, Codex systems integration, and more.
They converge.
After your intake, every expert reviews your substrate within their specialty. The orchestrator reconciles overlap, resolves conflicts, and produces one coherent plan — not 25 parallel chatbot answers.
They reconvene.
Every lab you upload, deep-dive you complete, routine you confirm, or wearable sync brings the panel back together. The plan refines, your Week Codex score climbs toward your Goal.
Ask any one of them.
Subscribers can chat 1:1 with any expert to discuss something that matters to you. Then if desired, the outcome of the conversation can be added to your plan with one click. This is real personalization!
Honest answers to the questions you\u2019re actually asking.
Is HRT safe for me personally? ▼
For most symptomatic women under 60 — or within 10 years of menopause — the benefits of HRT outweigh the risks. The 2002 WHI study scared a generation of women, but the original headlines overstated risk and understated benefit. The long-term WHI follow-ups, the NAMS 2022 position statement, and the FDA’s 2025 removal of the estrogen black-box warning confirm: timing, formulation, and your individual risk profile are what matter. A family history of breast cancer does NOT automatically rule HRT out — it changes the conversation, not the answer. TTL captures your risk factors and surfaces the specific questions to bring to your clinician.
Will HRT actually help with my hot flashes, sleep, brain fog, and low libido? ▼
Yes, for most women. HRT reduces vasomotor symptoms (hot flashes, night sweats) by 75–90% within 4–8 weeks. Sleep typically improves within 2–4 weeks as night sweats resolve. Mood and anxiety often stabilize within 2–6 weeks. Brain fog improves over 2–12 weeks. Libido is slowest — testosterone addition may be needed, with full effect in 4–12 weeks. Joint pain and body composition changes take 3–6 months. Your TTL Codex tracks these improvements weekly so you can see real progress, not just hope.
How long will I have to take HRT? What happens when I stop? ▼
There is no universal stop date. Current guidelines (NAMS 2022, IMS 2024) recommend individualized duration with annual review. Most women use HRT for 5–10 years; some continue indefinitely for bone, heart, and brain protection. The outdated “5-year rule” came from the original WHI reporting. If you stop: ~50% of women experience some symptom return (usually milder), and clinicians recommend gradual tapering over 3–6 months rather than abrupt cessation. Bone protection stops when HRT stops. You are not “dependent” — HRT replaces hormones your body used to make; stopping it returns you to where you’d be without it.
What are the common side effects of HRT? ▼
Most side effects occur in the first 1–3 months and resolve on their own: breast tenderness, bloating, headaches, spotting or breakthrough bleeding, and mild nausea (oral only). These typically indicate the dose needs adjustment, not that HRT is wrong for you. Serious side effects are rare and largely mitigated by using transdermal delivery (patch, gel, spray) instead of oral. Your TTL plan includes a side-effects timeline so you know what’s normal vs. what warrants a call to your clinician.
Will HRT cause weight gain? ▼
No. Menopause itself drives weight redistribution (especially visceral belly fat) due to declining estrogen. HRT may help prevent or partially reverse this shift. Some women notice mild fluid retention in the first 2–4 weeks, which resolves. Studies consistently show HRT users gain less abdominal fat than non-users over time.
What type of HRT is best for me — pills, patches, gels, or pellets? ▼
It depends on your risk profile, lifestyle, and preferences. Transdermal (patches, gels, sprays) avoids first-pass liver metabolism and carries no additional clot risk — it’s the default in most modern protocols. Oral is convenient but raises clot and gallbladder risk slightly. Pellets provide steady levels but are difficult to adjust. Your blueprint lays out the trade-offs for each form based on your history, and the Lane Rx clinician (coming soon) will prescribe what fits.
Is bioidentical HRT safer than FDA-approved HRT? ▼
The claim that compounded “bioidentical” hormone therapy is safer than FDA-approved therapy isn’t supported by current evidence. The FDA, The Menopause Society (NAMS), and the Endocrine Society don’t endorse it as safer. FDA-approved bioidentical options (estradiol patches, micronized progesterone) have strong safety data. Custom-compounded bioidenticals lack the same regulatory oversight and standardized dosing. The key distinction is delivery method and progesterone type, not the label.
Can I take HRT if I have a family history of breast cancer or blood clots? ▼
A first-degree family history does NOT automatically disqualify you. It changes which delivery method (transdermal strongly preferred), which progesterone formulation, and what monitoring cadence your clinician recommends. Many women with family history safely use HRT after an individualized risk-benefit discussion. Your TTL blueprint captures family history at intake and surfaces the specific literature and questions to bring to your clinician.
Are there natural alternatives or non-hormonal options? ▼
Yes. Phytoestrogens (soy isoflavones, red clover), adaptogens (ashwagandha, rhodiola, maca), targeted nutrition (cruciferous vegetables, ground flaxseed), and lifestyle interventions (sleep optimization, resistance training, stress management) are all in scope. For some women, lifestyle bedrock alone is enough. Your blueprint surfaces these strategies alongside or instead of HRT based on your stated preferences and risk tolerance.
When should I start HRT? Am I too young or too old? ▼
The optimal window is within 10 years of menopause onset or before age 60 — this is when cardiovascular and bone benefits are strongest. Perimenopause (while still having periods) is a valid and common starting point. Starting after 60 isn’t impossible but requires more careful risk assessment. Your TTL blueprint maps where you are on this timeline.
Do I need blood tests to qualify for HRT? ▼
Labs are helpful but not required to start. Menopause and perimenopause are diagnosed clinically (symptoms + cycle history), not solely by lab values. That said, estradiol, FSH, thyroid panel, vitamin D, and a metabolic panel sharpen the plan dramatically. Upload existing labs and we’ll parse and trend them for you.
Does TTL prescribe HRT? ▼
No — TTL never prescribes. TTL is the longevity-intelligence platform: read your labs, build the personalized blueprint, prep you for the clinician conversation. Lane Rx, when live, will match you with a licensed clinician — separate from TTL — who handles evaluation, prescription, and follow-up.
Which biomarkers should I track for hormone health? ▼
A typical baseline panel: estradiol, progesterone, FSH, LH, total and free testosterone, SHBG, AMH (if it’s relevant for your stage), a thyroid panel, vitamin D, ferritin, and a fasting metabolic panel. Your blueprint will tell you which ones matter most for you right now — based on your symptoms and where you are in the perimenopause-to-postmenopause arc.
When does the Lane Rx telehealth tier launch? ▼
We’re onboarding the clinician network now. App subscribers get priority access when Lane Rx opens. If you’d like a heads-up when it goes live, email hello@ttlongevity.com.
How we keep this honest.
Six commitments we hold ourselves to. They're also why we look different from the clinics.
Independent
No formulary, no kickbacks, no compounds for sale. Your protocol is the one that fits, not the one we're paid to push.
Encrypted at rest
PHI columns are encrypted at the application layer (AES-128 + HMAC) with a key held in our hosting provider’s encrypted secret store, separate from the database. Logs never contain raw PHI.
No data sales, no ads
We don't sell, rent, or trade your data. We don't run ads. Our revenue is the subscription you pay us — that's the entire business.
Independent guidance
High-quality health and wellness information intended to support informed decision-making. We give you the protocol; the prescription stays with your doctor.
Export & delete anytime
Your data is yours. Export it as JSON or delete your account in one click — we honor a 30-day undelete in case you change your mind.
US & MX coverage
Telehealth matched to where you live, units in your system (lb/kg, ft·in/cm, oz/ml).
Built for people who've outgrown spreadsheets.
You already know your TSH, your hs-CRP, and your VO₂ max. You've tried the apps, the wearables, and a notebook or two. TTL is the next step — a structured, expert-built protocol that connects what you're already tracking to what your plan should actually look like.
-
You ask better questions than your doctor's intake form does. So we ask better ones.
-
You want the protocol AND the reasoning. Every recommendation cites the mechanism and the evidence tier.
-
You'd rather pay $9.99/mo than be the product. No data sales, no ads, no upsell kickbacks.
A plan that meets you where you are.
Five minutes of intake. Real lab interpretation. A clinician-ready blueprint built around your stage, your symptoms, and what you actually want from the next thirty years. Free to start.